
Designing Breast Lift Scars
Many women want a breast lift, but they get understandably hung up on the subject of scars. I hear some version of this every week: “Can I just have the smaller scar?” or “Can you lift my breasts without that line down the middle?” I understand the concern completely. No woman comes into my office excited about having incisions placed on her breasts. At the same time, a breast lift is fundamentally a shaping operation, and shaping requires decisions about skin removal, breast support, and incision placement. That is the heart of the incision decision.
What I think patients appreciate most is honesty. I do not believe in pretending scars do not matter. They do. But I also do not believe the shortest scar is automatically the best operation. In breast lift surgery, the scar pattern is not the goal. The goal is a youthful, tasteful breast shape with the nipple in the right position, the lower pole controlled, the areola sitting attractively, and the overall breast proportion looking natural. The scar pattern is simply the tool I use to get there. If I choose the wrong tool because everyone is fixated on minimizing the incision at all costs, the breast shape may suffer, and that is usually not a trade patients are happy with in the long run.
In this breast lift page, this same philosophy comes through clearly. There are several breast lift techniques, including the Wise pattern, the lollipop pattern, the periareolar technique, and the crescent technique, and the operation is tailored to the patient’s anatomy. Some women may need implants if volume has been lost, while others may pair the breast lift with other procedures, such as a tummy tuck, for a more complete transformation. That is important context because breast shape is not created by the incision pattern alone. Volume, tissue quality, nipple position, and skin excess all affect what kind of lift makes sense.
The Two Most Common Breast Lift Scars
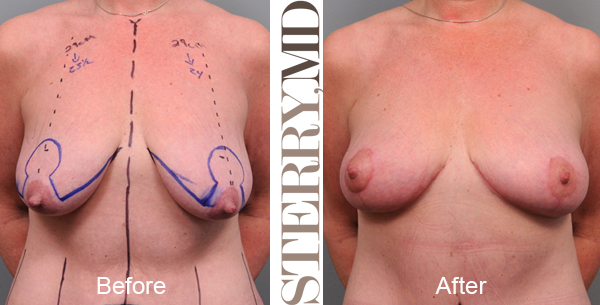
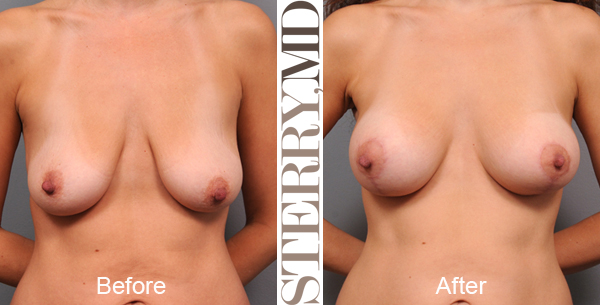
As the live article explains, there are many techniques in breast lift surgery, but in practical terms the two most common scar patterns I discuss with patients are the “Lollipop Breast Lift Scar“ and the “Anchor Breast Lift Scar“, which are shown below. The lollipop pattern circles the areola and extends vertically down the center of the lower breast. The anchor pattern includes those same components and adds a scar hidden in the breast crease. Both are well-established operations, and both can produce beautiful results in the right hands on the right patient.
The lollipop lift appeals to patients for obvious reasons: it avoids the longer scar in the fold under the breast. For the right anatomy, it can do an excellent job. I use it often, and I like it very much when the skin excess is moderate, the tissue is cooperative, and I believe I can get a pleasing shape without needing more horizontal skin removal. On this site’s gallery and procedure pages, you can see multiple cases where the lollipop pattern works very well, especially in women who need a lift but do not have extreme skin redundancy.
The anchor lift, on the other hand, is extremely useful when there is more skin to remove or when the breast needs more comprehensive reshaping. Patients sometimes hear “anchor” and assume it must be the old-fashioned or inferior choice simply because it involves an additional scar. I do not see it that way at all. The anchor pattern can be a more elegant operation when it allows me to control the lower pole better, tighten the skin envelope more effectively, and create a more stable, attractive breast. My photo gallery explicitly shows anchor-lift examples in women who had more skin excess, including after significant weight loss, and notes that it can restore a more youthful breast shape very nicely.

Both of these techniques can yield beautiful results if performed well on the right candidates. There have been many academic papers written that try to define specific parameters and dictate when either operation can be performed, but I think this is more of an artistic issue.
I don’t have any hard and fast rules about when I do either one; it’s more of a sense I get from the physical examination of each breast. The goal in my mind is to get the best cosmetic outcome possible, not necessarily to force the patient’s anatomy to conform to any particular surgical plan. Of course, the patient always has the final vote on which operation we do.
Visor Flap To Avoid The Vertical Scar
The vertical scar is the one most women object to at first, and I understand why. It is the scar they imagine seeing when they look straight at the breast. Ironically, it is also one of the most useful scars in creating a good breast contour. By gathering and shaping the breast vertically, I can create projection, tighten the lower pole, and help the breast look rounder and more youthful. So yes, patients may dislike that scar in theory, but in practice, it is often central to getting a result they will like. The live article makes this same point very directly.
However, there is an operation designed that does NOT use that incision. The visor flap is a technique designed to avoid that vertical component. But it is a very specialized operation, not a general solution for ordinary breast lift patients. It is rarely used and mainly useful in women seeking Breast Reduction whose breasts are very large and whose nipples rest far below the inframammary crease. That is a very specific anatomy. It is not what the average woman seeking a mastopexy presents with.
I tinkered with this method a few times back in the early 2000’s, but I was never truly satisfied with the cosmetic outcomes. Furthermore, the number of people who fit the requirements is very small. This procedure has largely fallen by the wayside. My friend and colleague, Dr. Allan Parungao, was more persistent than I and managed to get the operation to work with some very good success. I have one of his cases presented here:

Some surgeons develop more comfort and better outcomes with niche techniques than others. But I think the more important takeaway for patients is not that there is some scar-free or scar-sparing trick being withheld from them. It is that every technique has indications, limitations, and tradeoffs. If a procedure avoids one scar but gives a less satisfying shape in the average breast lift candidate, then it is not really solving the problem most patients came in to fix.
So when a patient asks me, “Do I have to have that scar down the middle?” my answer is usually that the question is not whether I can avoid it in theory, but whether avoiding it helps or hurts the final breast shape in her case. In most routine mastopexy patients, the vertical component is helpful enough that trying to sidestep it becomes more of a compromise than an advantage. I think patients appreciate that explanation once they see before-and-after photos and understand what that scar is actually doing for them.
Understanding Breast Lift Surgery
I try to help patients make this choice by explaining the issues. I show them many before-and-after photos of other women, I draw diagrams, and show graphics that are typically used for teaching residents how these operations are done. Breast lift surgery is not something patients should choose by buzzword. “Lollipop” and “anchor” are shorthand labels, not treatment plans. A real plan comes from examining the breasts, understanding what the patient wants, and being honest about what can and cannot be achieved.
For example, some women come in wanting a breast lift when what they really want is upper-pole fullness. A lift alone can give me fullness behind the nipple and improve nipple position, but in this breast lift page, I explain very clearly that if a patient wants true fullness above the nipple, implants may be necessary. That is a critical distinction. If I promise the wrong thing, or if the patient hears “lift” and imagines the look of an augmented breast, disappointment becomes much more likely. Understanding the operation means understanding not just scars, but shape, volume, implant needs, and realistic outcomes.
Once the patient has a better understanding of their own personal anatomy and can verbalize what they want after the breast lift, then we can create a surgical plan. Rarely, I have to tell them I can’t deliver the results that they want based on the limitations that they put in place on size and or breast lift scar placement. If they are unrealistic about what plastic surgery can do for them, then it’s best that we don’t work together. Sometimes I wish I were back in liposuction, where patients only generally ask about the cost of liposuction and the time required to recover. Gone are the simple days for me. Breast lift conversations are nuanced because they involve aesthetics, anatomy, scars, and expectations all at once. They require more visual education than many patients anticipate. But that is exactly why I take the time to show before-and-after galleries, including cases of breast lift alone, and breast lift with implants, so the patient can see how different scar patterns behave in real women.
Breast Lift Training Is Sometimes A Factor
Some of these decisions are dependent on the training of the surgeon. There are “purists” who believe surgeons should ALWAYS do one technique or the other. I find that the words “always” and “never” are rarely the right answer on the exam… or in life. I was lucky to have trained during a time that both major incision styles were being used. It enables me to do either operation with proclivity. The only question is which one I think is best suited to the patient attached to the breasts in question.
Breast Lift Scar FAQs
Can breast lift scars look worse before they look better?
Yes, and that often surprises patients. Early scars can look pink, firm, slightly raised, or more noticeable than expected, but that does not mean they are healing poorly. In most cases, they soften and fade gradually over many months.
Why do some breast lift scars look faint even when they are longer?
Length is only one part of how visible a scar feels. A longer scar that is thin, flat, and placed in a natural contour, such as the inframammary fold, can be less bothersome than a shorter scar that widens or distorts the breast shape. Patients usually respond more to the overall look of the breast than to scar length alone.
Can choosing the “smallest scar” actually make my breasts look less lifted?
Yes, it can. If I limit the scar pattern too aggressively in a patient who needs more skin removal, the result may be a breast that still looks elongated, loose, or under-corrected. A slightly more extensive incision can sometimes create a much more attractive and durable shape.
Why do patients often worry most about the vertical scar before surgery?
The vertical scar is the one patients imagine seeing straight on when they look in the mirror. Ironically, it is also one of the scars that often heals better than expected and contributes the most to shaping the breast. Once patients see how much it helps the contour, they are usually less bothered by it than they expected.
Can breast lift scars stretch if I gain or lose weight later?
They can. Significant weight changes alter the skin envelope and can place new tension on the breasts, which may affect both shape and scar appearance over time. That is one reason I prefer patients to be at a stable weight before surgery.
Do scar patterns affect how natural the breast looks in clothing?
Absolutely. The scar itself is usually hidden in clothing, but the incision pattern determines how much shaping I can achieve. In everyday life, patients usually notice the improved position, support, and silhouette long before they think about the scar lines.
Can my scar choice affect whether I may need a revision later?
Potentially, yes. If a scar pattern is too limited for the anatomy, the breast may not be shaped as well or may settle in a less attractive way over time. In that situation, a patient may later wish she had accepted the more appropriate incision pattern from the beginning.
Worried About Breast Lift Scars? Let’s Talk About What They Really Look Like
If breast lift scars are the one thing holding you back, the best next step is a thoughtful consultation. Schedule a private consultation with me, so that I can evaluate your anatomy, explain which incision pattern makes the most sense for your breasts, and show you what those scars typically look like once they heal. The goal is not just fewer scars. It is a better breast shape with scars that are worth the tradeoff.



Leave a Reply